
When the 25-year-old woman enrolled in a longitudinal study on obesity in 2016, she was healthy by all standard measures, with one exception: her body mass index (BMI). As is the norm for study participants, her identity is protected, but let’s call her Mary. At 215 pounds, Mary had a BMI—a metric based on height and weight—that put her squarely in the “obese” category. Yet she didn’t have health problems associated with obesity, such as high blood pressure, elevated levels of cholesterol and other blood lipids, or a prediabetic condition called insulin resistance. Five years later Mary had gained 68 pounds, but her vital signs and blood work showed her to be healthy even as her BMI rose enough to categorize her as extremely obese.
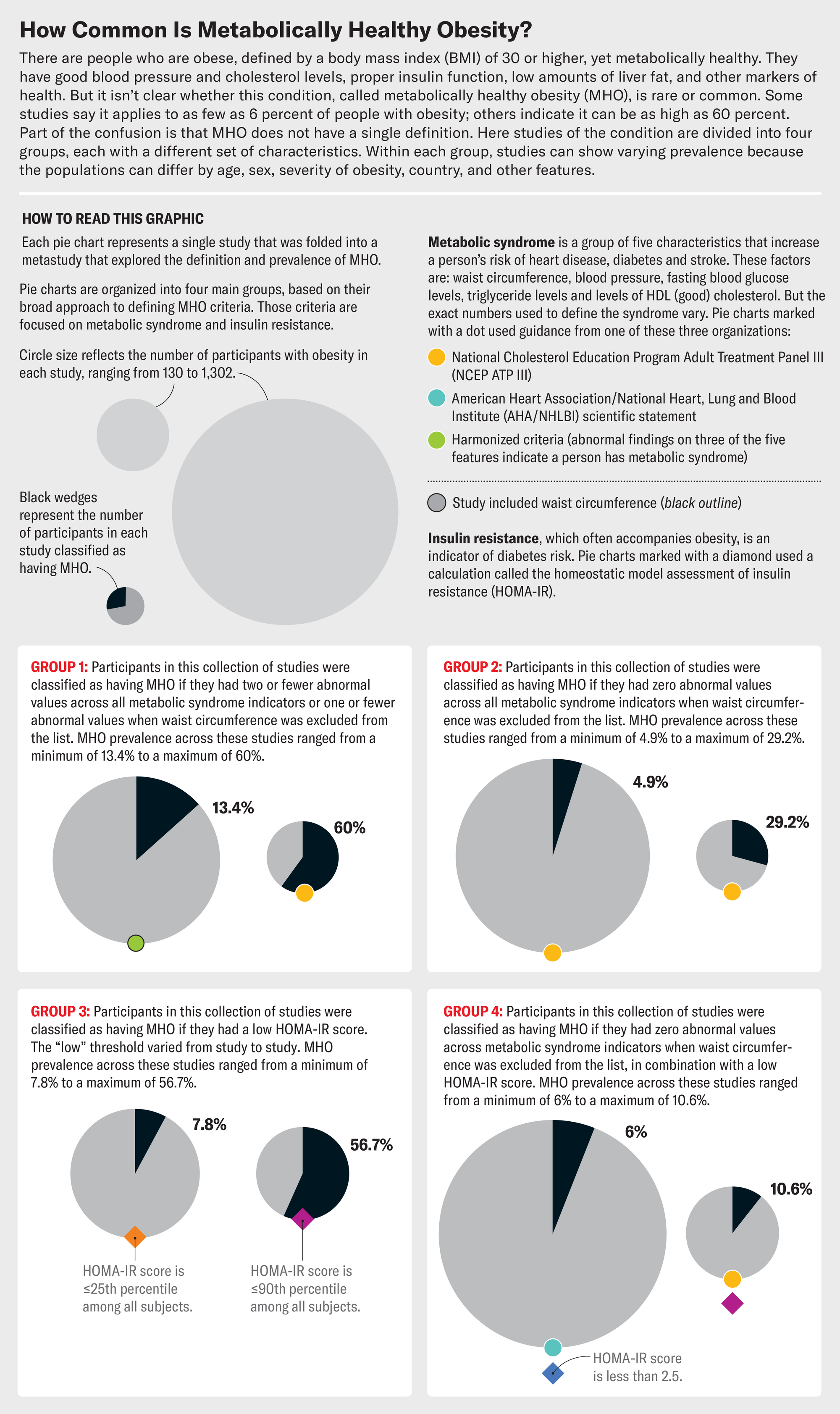
Mary is not alone. Although people with more body fat are at increased risk of health conditions such as diabetes, heart disease, stroke and some cancers, studies have repeatedly identified a subset of people with high BMIs and good metabolic health. Their blood pressure, cholesterol levels, insulin sensitivity, triglyceride counts, liver fat levels, and more are good. Researchers call this phenomenon metabolically healthy obesity (MHO). Depending on how it’s defined, the condition fits as few as 6 percent or as many as 60 percent of adults classified as obese according to their BMI numbers. (People with BMIs between 25 and 29.9 are considered overweight, and those with values higher than 30 rate as obese.) They are heavy, but they are healthy.
The identification of people with metabolically healthy obesity suggests obesity may not automatically lead to illness.
On supporting science journalism
If you're enjoying this article, consider supporting our award-winning journalism by subscribing. By purchasing a subscription you are helping to ensure the future of impactful stories about the discoveries and ideas shaping our world today.
The identification of people with MHO suggests—controversially—that obesity may not automatically lead to illness and that the health risks associated with it may be overstated. MHO has been embraced by a movement that says a person can be healthy at any size: patients and physicians who push back against the stigma and stereotyping that society and the medical establishment have attached to people with bigger bodies. It also ties in with mounting criticism of the accuracy and usefulness of BMI as a measure of health. “I’ve found that BMI has not been that helpful in predicting who’s at risk of disease among my patients,” says Mara Gordon, an assistant professor of familymedicine at Cooper Medical School of Rowan University in Camden, N.J.
MHO is contentious because it challenges the idea, drawn from many studies and decades of research, that the risk of serious illness rises with obesity. What’s more, losing weight has been shown to improve many conditions, including diabetes, high blood pressure, elevated blood lipids, obstructive sleep apnea and osteoarthritis.
Obesity is “not a cosmetic issue. It’s not about size,” says Alyson Goodman, a medical epidemiologist in the Centers for Disease Control and Prevention’s Division of Nutrition, Physical Activity and Obesity. “We’re worried about the risk for serious chronic diseases over time.” Some researchers contend that MHO is merely a temporary state obese people may pass through on the way to developing health issues commonly connected to a higher body weight.
Still, Mary and others like her are proof that people can be obese but medically healthy for many years. Other research has found that being a bit overweight is not as dangerous as previous guidance suggested and may even be protective. Recent work on the physiology of fat shows that it’s not always a problem. More and more evidence suggests it’s time to reconsider standard assumptions about weight and health.
Samuel Klein, a physician and obesity expert at the Washington University School of Medicine in St. Louis, and his research group have identified people who are obese but seem to be resistant to obesity-related metabolic effects. Klein cautions that “it’s a very small percentage of obese people who are truly metabolically healthy,” but he says it’s a real phenomenon. And his studies aren’t the only ones to find it. People with MHO have been identified in many cohorts, but it’s hard to know how common it really is because different studies have used different criteria for classifying MHO. “There are more than 30 different definitions in the literature,” Klein says, “so it can be really misleading.”
One of the most extensive studies of MHO examined data from NHANES III, a representative survey of more than 12,000 people in the U.S., and determined that MHO was best categorized based on three criteria. One is blood pressure (systolic blood pressure—the first of the two numbers you get when your pressure is measured—less than 130 millimeters of mercury, or mm Hg, without medications). The second is waist-to-hip ratio (less than 0.95 for women and less than 1.03 for men). And the third is the absence of type 2 diabetes. Using these criteria, the researchers calculated that 41 percent of participants in the NHANES III cohort with obesity could be considered as having MHO. The scientists also applied them to people in the UK Biobank database and found that 19 percent of obese participants in that cohort of more than 374,000 people had MHO. Under these criteria, MHO was not associated with any greater risk of death from cardiovascular disease or other causes compared with a “normal weight” group, says the study’s senior author, Matthias Schulze, a molecular epidemiologist at the German Institute of Human Nutrition Potsdam-Rehbrücke in Nuthetal.
Jen Christiansen; Source: “Metabolically Healthy Obesity: Facts and Fantasies,” by Gordon I. Smith, Bettina Mittendorfer and Samuel Klein, in Journal of Clinical Investigation, Vol. 129; October 2019 (data)
But were all these people truly metabolically healthy? It depends on how you define MHO. Schulze and his colleagues examined three other common definitions and found that fewer than 6 percent of the NHANES III participants in their study met the criteria for all three, with the range going from just under 10 percent for the strictest definition to nearly 47 percent for a definition that allowed up to two of five possible metabolic symptoms to be present.
Although some people clearly have MHO, researchers disagree about whether it persists or is just a temporary state. A study of more than 4,000 adults in Australia found that about 12 percent of them had MHO, but about a third of those people became metabolically unhealthy over the course of the five- to 10-year follow-up. An analysis of more than 4,000 participants in the long-running Framingham Heart Study found that almost half of people categorized as having MHO at one point in the longitudinal study no longer did by the next examination cycle, four years later. And a study of British government workers over two decades found that slightly more than a third of the study’s obese participants had MHO at baseline, but after 10 years, 35 percent of them had stopped meeting the criteria, and after 20 years, 48 percent were no longer healthy enough to be categorized as having MHO. These studies all suggest that MHO doesn’t last for everyone. But looked at a different way, the studies also show that a substantial number of obese people—often more than half—maintained metabolic health for many years.
Klein’s group has identified people who, like Mary, fit the most stringent definitions of MHO and appear to resist the adverse effects of weight gain and higher body fat percentage on their cardiovascular and metabolic systems over time. Researchers are eager to understand exactly what it is that protects them.

Ni-ka Ford; Sources: “Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications,” by Michele Longo et al., in International Journal of Molecular Sciences, Vol. 20; May 2019, and “Targeting Adipose Tissue in the Treatment of Obesity-Associated Diabetes,” by Christine M. Kusminski et al., in Nature Reviews Drug Discovery, Vol. 15; June 2016 (references); Jeffrey Horowitz (consultant)
There are some clues. People with MHO are typically women who carry their fat mainly in their buttocks and hips while having a narrow waist, Klein says. Their fat tissue seems to function in a way that’s protective. Their bodies are sensitive to insulin. Compared with people with metabolically unhealthy obesity, they have higher levels of physical fitness and lower body fat percentages. Ethnic background also matters. People of South Asian, East Asian, Chinese or Japanese descent tend to have metabolic complications at a lower BMI or body weight than people of other ancestries, Klein says.
How fat is stored in the body may explain some of these findings. Excess lipids can collect in internal organs and disrupt their functioning—a phenomenon known as lipotoxicity, says Daniel Cuthbertson, a physician in cardiovascular and metabolic medicine and a professor at the University of Liverpool in England. This fat can induce insulin resistance, or it may incite chronic inflammation or scarring in the organs. “A small amount of fat deposition within the liver and a small amount within the pancreas can make a huge difference to someone’s metabolic state,” Cuthbertson says. This is true whether the person has obesity or not, he says. People with low BMIs can also have many of the health issues associated with obesity if fat is stored in their organs.
Why some people have health problems and others at a similar weight don’t may be explained by something called a personal fat threshold—how much fat your body can deposit in subcutaneous fat stores (the fat right underneath your skin) before it moves to sites such as the liver and the pancreas where it causes problems, Cuthbertson says. “Different people have different personal fat thresholds,” he says. People with South Asian ancestry, he says, “probably have a lower personal fat threshold because when they gain weight, they don’t need to gain as much weight to develop more severe health consequences.”
“Fat tissue is fantastic,” says Jeffrey Horowitz, a professor at the University of Michigan, who studies exercise and metabolism. It’s a complex mix of different cells intermeshed with a protein matrix, which forms a kind of net that holds the tissue together. The vast majority of our fat is stored subcutaneously, and that’s generally the best place to have it, he says. “If you’re going to be storing fat, you want to be storing it there and not in your visceral region.” Fat in the thighs is better than fat in the belly. One key feature of obese people with metabolic impairment is that they’re no longer able to store fat effectively in subcutaneous regions, so excess amounts go into the circulatory system and cause problems elsewhere. “If you can increase your capacity to store it, that would be great,” Horowitz says. Some drugs that do exactly that—expand subcutaneous fat tissue’s storage capacity—can be used to temper the symptoms of diabetes or prediabetes, he says.
“The specter of death is always presented to me as a part of my health profile because of my body size.” —Tigress Osborn National Association to Advance Fat Acceptance July/August
When entering middle age, most healthy, active people gain body fat. But their risk of developing diabetes will be lower if they have small fat cells that can expand effectively and have sufficient vasculature to feed the fatty tissue, Horowitz says. “Some people innately have that capacity,” he adds. He likens it to an expandable suitcase that is normally zipped closed but has the ability to expand if you find yourself with extra cargo. Fat tissue in people with MHO seems to be adept at this scale-up.
The recognition that it’s possible to be heavy and metabolically healthy may help the push to destigmatize larger bodies and acknowledge that bigger is not bad. “The idea that people are fat because they are lazy and greedy is still pervasive,” says Tigress Osborn, executive director of the National Association to Advance Fat Acceptance. The evidence emphatically shows that these biases are false. “Body weight regulation is extremely complex and involves many biological pathways and factors beyond just what we eat or how much we exercise,” says Rebecca Puhl, professor of human health and family development at the University of Connecticut. “Many of these factors, like genetics, environment and biology, are outside of personal control,” she adds. Yet fatness has become a medical category, Osborn says, rather than just “a physiological difference between people.” Instead of recognizing natural variation in body sizes and shapes, we label fatter bodies as diseased, she says.
In medical settings, larger-bodied people are constantly bombarded with the message that their fat is slowly and surely killing them, Osborn says, “even when you are a fat person who has none of the markers [of ill health].” She adds that “the specter of death is always presented to me as a part of my health profile because of my body size, regardless of what my numbers say. At what point do I ever get to be designated as healthy?”
Weight stigma itself is a public health issue, Puhl says. “When a person is shamed, stigmatized, treated unfairly or bullied because of their body size, this increases their level of psychological distress,” she explains. It also ups the risk of depression, anxiety, low self-esteem, poor body image, and even suicidal thoughts and risky behaviors such as substance use. Stigma can become a form of chronic stress that can increase cortisol levels and cause physical harm—and weight gain. Studies show that weight discrimination and bias are common in health-care settings, which can discourage heavier people from getting needed medical help. Bias on the part of health-care providers can also interfere with proper diagnoses when doctors assume their patients aren’t sick and just need to lose weight, Puhl notes. Repeatedly going on and off diets—yo-yo dieting—can cause major health problems.
Obesity’s status as a disease was formalized in a resolution passed in 2013 by the American Medical Association’s house of delegates. Douglas Martin, medical director of occupational medicine at CNOS in Dakota Dunes, S.D., chaired the AMA committee that heard testimony on the resolution. There were two main drivers behind the effort, he says. The biggest one was that physicians were having difficulty getting certain tests and treatments for obesity covered by insurance carriers. “You couldn’t treat obesity in and of itself. It had to be in concert with diabetes, hypertension, joint problems, etcetera,” Martin says. The second driver was a growing concern that obesity was becoming epidemic in the U.S. The most current statistics from the CDC show that nearly 42 percent of adults in the U.S. have BMIs that classify them as obese.
The resolution was adopted, after some vigorous debate. The AMA’s Council on Science and Public Health recommended against the measure. “Just being of increased weight, if there’s no other impaired function, doesn’t fit any of those definitions of a disease,” council member Robert Gilchick told MedPage Today at the time. He objected to giving a disease label to apparently healthy people, asking, “Why should a third of Americans be diagnosed with a disease if they’re not necessarily sick?” Others on the council worried that people with obesity who improved their diet, physical activity and sleeping habits would still be identified as “diseased” and pressured to get treatment if they failed to change their BMI classification.
Some people in the health field hoped that declaring obesity a disease would reduce stigma in some ways, by conveying the idea that it is a medical condition rather than a personal failing. But Osborn says that the designation has also led to mixed messages. She asserts that “it makes fat people feel like their doctors are blaming them for not treating their disease correctly.” Even worse, “we’re only going to talk about you as a disease now, and we’re only going to talk about your body as a medical condition, as though there are no other aspects to living in the human body.”
Turning obesity into a disease essentially meant declaring that larger bodies are abnormal and unwell. To Osborn’s question, “At what point do I ever get to be designated as healthy?” the answer from the medical establishment was: never (unless you make yourself smaller).
One major objection raised to declaring obesity a disease is that its basic diagnostic measure may not be meaningful. The standard for measuring obesity is BMI, in part because it is easy to gauge, is inexpensive and, at a population level, correlates well to body fat levels. But it’s an imperfect metric. Actor Dwayne “The Rock” Johnson has a BMI of around 34, “but he’s not obese—he’s a very muscular kind of guy,” Klein says. On the other end of the spectrum, he says, “you can have people with a normal BMI who are very doughy, and they have a high body fat percentage.” Ideally, obesity should be based on the percentage and location of that fat, Klein says, as well as any medical complications present, “but again, we don’t have good cutoffs.”
The current system of BMI classification is, in fact, totally arbitrary, says epidemiologist Katherine Flegal. Now a consulting professor at Stanford University, Flegal spent nearly 30 years at the CDC’s National Center for Health Statistics. Flegal says the BMI cutoffs for healthy, overweight and obese are not based on solid research. In 2005 she and her colleagues published an analysis of U.S. population statistics showing that people classified as overweight (BMI of 25 to 29.9) actually had lower death rates than people in the “healthy” category. In 2013 she and several collaborators published a review pooling data from 97 studies from around the world, with more than 2.8 million people, that showed the same thing.
Flegal says her work doesn’t show that fat is harmless, but it has been attacked by different scientists in this area. And other large studies have contradicted her findings. For instance, in a multistudy analysis published in 2016, researchers examined records from 3.9 million people and found that death rates went up consistently as BMI classifications rose from healthy to severely obese.
All these studies on the link between BMI and mortality—both its pros and its cons—suggest that this entrenched metric does not measure the things that matter most about health and that the relationship between BMI and health is not straightforward. The medical community is beginning to accept this criticism of the ubiquitous measure. In 2023 the AMA adopted a new policy and stated that BMI is “an imperfect way to measure body fat in multiple groups given that it does not account for differences across race/ethnic groups, sexes, genders, and age-span.”
The links between weight and health become even more complex when researchers look at weight loss. “We don’t really understand why losing weight is so beneficial,” Klein says. People with obesity and metabolic problems who lose 5 percent of their body weight often show marked improvements in health measures, and more loss is better up until around 15 to 25 percent of the person’s starting weight, where the benefits may max out, Klein says. It’s not clear why.
But losing weight does not always improve health. The Look AHEAD study was a large-scale clinical trial that tested whether an intensive, lifestyle-based weight-loss intervention could reduce the incidence of cardiovascular events in overweight or obese adults with type 2 diabetes. The trial, which included more than 5,000 people, was halted early because although the participants receiving the intervention did lose more weight than those in the control group, they did not show a reduction in cardiovascular problems.
Losing fat is no easy task. Many decades’ worth of evidence demonstrates that most efforts to lose weight through diet and exercise fail. New drugs such as Ozempic and Wegovy that work by mimicking the hormone GLP-1 (glucagonlike peptide 1) are producing weight loss at levels never before seen from a medication, but they’re extremely expensive and in short supply. And some of the people who could benefit the most won’t have access, which could make issues of health equity even worse.
When people stop taking these drugs, the weight comes back, so patients may need to be on them for life. The drugs also don’t work for everyone, and they come with side effects that could make it hard for some to take them over the long term. All of this means that many people are going to continue living in bodies that are larger than the medical (or social) ideal. Is it possible for them to be healthy in the bodies they have?
The evidence points to a qualified yes. Body weight and shapes exist on a continuum, and the extreme ends of the continuum—being medically very underweight or extremely obese—do seem to come with a high risk of health problems. But there’s a lot of variation and nuance.
The British Dietetic Association assessed the evidence on BMI and health for a 2023 report offering food and nutrition advice for adults aged 65 and older. “One of the pieces of advice is don’t worry if you’re a bit overweight,” says Mary Hickson, a professor of dietetics at the University of Plymouth in England, who was involved in the report. The researchers found that in older adults, the range for healthy weight is wider than assumed: instead of a BMI of 18 to 25, it can be up to 28 or 29. Why the change? “I don’t think anybody’s really certain,” she says. One theory is that fat reserves are beneficial—having a little stored gives you some energy to call on if you get sick.
Some people do have high levels of fat without health consequences. But it’s clear that certain types of fat are detrimental.
There’s also the fact that body composition changes with age. “When you hit about age 40, you start to very slowly lose lean tissue, which is primarily skeletal muscle,” Hickson says. Body composition slowly shifts to less lean and more fat mass, and this change becomes more pronounced in a person’s mid-60s and 70s. The studies Hickson’s group reviewed showed a connection between being slightly overweight and having lower death rates than underweight groups. “It could be that you’re better able to maintain your muscle mass the more weight you carry in your body because people who are obese do have higher levels of muscle,” Hickson says. For these older people, the report’s takeaway message was to enjoy eating and not worry too much about being a little overweight.
But separately from metabolic health, excessive weight can raise certain disease risks as time goes on. People with MHO are still at risk of biomechanical complications from obesity, such as sleep apnea, osteoarthritis, gastroesophageal reflux, urinary incontinence, and other consequences of carrying a large body mass over the years, says W. Timothy Garvey, an endocrinologist at the University of Alabama at Birmingham. “They’re not going to get a free ticket from that perspective.”
Cancer is another danger that comes with all types of obesity. “There’s very good evidence that the risk of probably 15 different cancers is significantly increased,” Cuthbertson says. The mechanisms aren’t clear, but one theory is that it’s driven by hormonal changes associated with obesity. Fat tissue also can secrete biochemical signals that may promote the growth of tumor cells. Another hypothesis is that fat tissue can cause inflammation that may exacerbate cancer.
Dementia is also more common. Dementia risk is increased in people who have insulin resistance, and people who’ve been living with obesity and insulin resistance are at added risk for developing cognitive dysfunction and dementia later in life, Klein says—a condition sometimes called type 3 diabetes.
So where does this leave us? The study of metabolically healthy obesity shows that the relationship between body fat and disease is complicated. Some people really do have high levels of body fat without bad health consequences. But it’s pretty clear that certain types of fat, such as the fat tissue surrounding internal organs, are detrimental. “If you are obese, losing a little bit of weight has significant health benefits,” Klein says.
Yet it’s hard to lose weight, and it’s impossible to target specific places in the body for that weight loss. And given how harmful fat stigma can be, focusing on weight may do more harm than good, says Gordon, the New Jersey physician. Rather than encouraging her patients to conform to an idealized weight or body type, Gordon focuses on things such as blood pressure, insulin resistance and lipid numbers. These conversations, she says, have nothing to do with the number on the bathroom scale. They’re about preventing complications from diabetes or joint pain or helping people sleep better. “If a patient has evidence of glucose intolerance, we talk about that. Some of the best ways to prevent diabetes are regular exercise and reducing sugar in the diet. So we talk about that.”
JoAnn E. Manson, an endocrinologist and epidemiologist at Harvard Medical School, says that after spending years studying obesity, she has concluded that emphasizing the digits on the scale is not as helpful as working toward a healthy, active lifestyle; instead it can become part of the problem. People who’ve been told they must lose weight for their health and try unsuccessfully to do so may feel a sense of despair.
Manson says the focus should be not just on pounds but also on all the things we already know we should be doing: eating diets higher in fruits, vegetables and whole grains; engaging in regular physical activity; and spending time outdoors. “If people are following a healthy lifestyle, and they’re less preoccupied with a number on the scale, they’re also less likely to feel stress and anxiety about their weight,” Manson says. Reducing stress and anxiety around body weight issues can in itself contribute to better health.
The latest obesity research offers a hopeful message—that health isn’t just about what the scale shows. Feeling comfortable, safe and accepted in one’s body is important, too. Health-care providers who treat heavier patients with respect and attention, rather than blaming all their medical issues on weight, can help people of any body size manage their health. Increasing knowledge about the effects of different types of fat, in different locations, may lead to better assessments of what is worrisome and what is not. Being well is about more than your body size. It’s about how you care for it.